Pharmacy First Toolkit: Urinary tract infections
Sonya Reuther,
04 Feb 2025![]() 10 Min
10 Min
Sonya Reuther,
04 Feb 2025![]() 10 Min
10 Min
Sonya Reuther,
04 Feb 2025![]() 10 Min
10 Min
Key information from patient history
Emergency or GP referral (direct referral to A&E if severely ill)
The Pharmacy First service in England allows community pharmacy teams to complete episodes of care for seven common conditions. This toolkit provides an overview of the clinical pathway and PGD used to deliver consultations for uncomplicated urinary tract infections in women plus essential information on the assessment, diagnosis and management of this condition.
After completing it, you will be able to:
Download the Toolkit PDF here.
Urinary tract infections (UTIs) are common in primary care and often patients will attend a pharmacy suspecting that this is their problem. This is especially true when they have a classic urine, urgency and suprapubic pain.
Although cystitis is often caused by a bacterial infection, it may also be from a non-infectious cause.
Bacterial infection is reported to be found in 50 per cent of cases, most commonly caused by Escherichia coli, often from the gastrointestinal tract.
An ‘uncomplicated’ UTI is defined as occurring in women who are otherwise healthy and with normal kidney function.
Non-infectious causes of cystitis include sensitivity to chemicals in products such as bubble baths, shower gels, feminine hygiene sprays or spermicidal jellies. These may develop a reaction within the urethra or bladder, causing inflammation and ‘chemical cystitis’.
About half of all cases of cystitis will resolve within three days, even without treatment. The challenge is to exclude a complicated from an uncomplicated UTI and to ensure that no red flag issues cloud the presentation. Use the clinical pathway for UTIs to help guide your diagnosis.
Acute, uncomplicated UTIs usually resolve within a few days with or without antibiotic treatment. Using an antibiotic to which the infection is sensitive may shorten the episode by 1.6 days (from 4.9 to 3.3 days) and may prevent complications.
Up to one in four women with a UTI has a recurrent infection within three to six months and over 40 per cent within 12 months, so advice on preventing recurrence is important.
Using target resources for UTIs will support consistent decision making and provision of advice in primary care and pharmacy in particular.
Uncomplicated urinary tract infections (UTIs) are one of the commonest infections in women between the ages of 16 and 64 years presenting in primary care.
The term ‘cystitis’ is frequently used to signal urinary symptoms and includes both infectious and non-infectious causes.
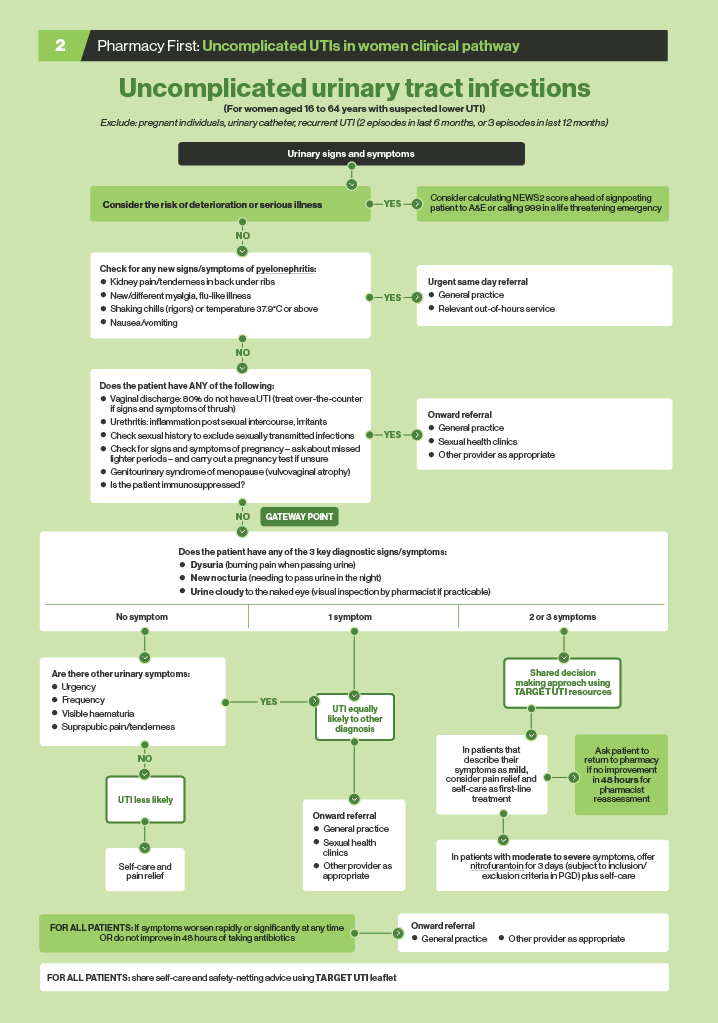
The three key diagnostic signs/ symptoms for UTIs are:
Note: In cases of uncomplicated UTIs in women, it is no longer routine to send urine for culture (although this is still necessary in pregnant women and those who are 65 years or older and who would be referred under the Pharmacy First service).
Download a PDF of the UTI clinical pathway here or see below:

The three key signs and symptoms considered to indicate urinary tract infection are:
TARGET/NHS advice is that the presence of two or more of these, with the absence of vaginal discharge, means a UTI is more likely.
Reflection exercise: Have a look at the TARGET antibiotic toolkit hub on the e-learning section of the Royal College of General Practitioners website. Click on the UTI resources tab and go to the Treating Your Infection leaflet. Discuss with members of your team how you will use the top half of the leaflet with a patient to assess the likelihood of a UTI and decide next steps depending on how many of the three key symptoms/signs the woman is experiencing.
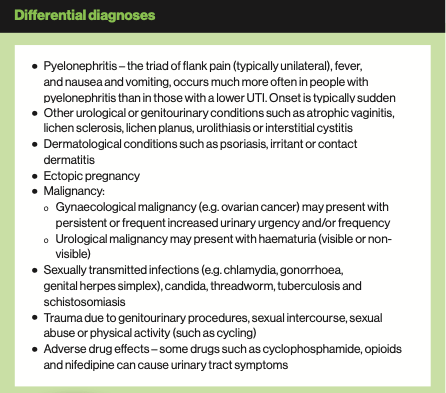
Systemic involvement, demonstrated by fever, chills, nausea, vomiting, loin pain and tenderness, is indicative of more serious infection, such as pyelonephritis, involving the upper urinary tract. Patients with these symptoms require urgent referral because of the risk of septicaemia. Back pain may also indicate an upper UTI.
Determining whether the patient is feverish can, to some extent, be done by observation and asking them. Taking the patient’s temperature will give a more accurate assessment.
Pharmacists can use the TARGET leaflet Treating Your Infection – Urinary Tract Infection (UTI), which is designed to be used jointly by health professionals and patients, to assess symptoms and discuss recommended care.
Age: The NHS Pharmacy First service in England is for women aged 16-64 years old. The reason for the lower age limit is that UTIs in children may result in damage to the kidneys or bladder, or may be caused by an abnormality of the urinary tract (such cases need investigating). Older women are more likely to have incidental bacteria and comorbidities that may complicate a UTI, so may present with confusion and weakness in addition to typical symptoms.
Female/male: Cystitis is more common in women than in men because bacteria need to pass up the urethra to enter the bladder. The urethra is much shorter in females than in males, so the passage of bacteria is much easier, and the process may be facilitated by sexual intercourse. There is also some evidence that prostatic fluid has antibacterial properties, which provides an additional defence against bacterial infection in males.
(Note: any man presenting with symptoms of cystitis requires medical referral because of the possibility of more serious conditions, such as kidney or bladder stones or prostate problems.)
Pregnancy: Any pregnant woman who presents with symptoms of cystitis needs referral because bacteriuria (presence of bacteria in the urine) in pregnancy can lead to kidney infection and other problems.
Development of symptoms: Cystitis sufferers often report that the first sign of an impending attack is an itching or pricking sensation in the urethra. The desire to pass urine becomes frequent: the woman may feel the need to pass urine urgently, but passes only a few burnings, painful drops. This frequency of urination occurs throughout the day and night (nocturia).
Dysuria (pain on passing urine) is a classical symptom of cystitis. After urination, the bladder may not feel completely empty and even straining produces no further flow. The urine may be cloudy and strong smelling.
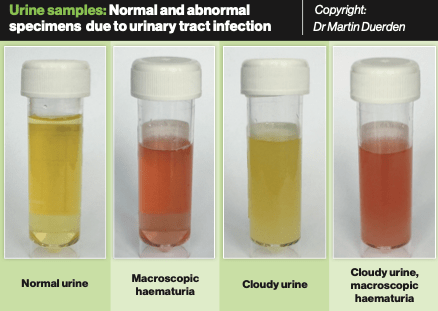
Blood in urine: macroscopic haematuria (visible presence of blood in the urine) is an indication for referral to the GP. It occurs in UTIs when the bladder lining and urethra are so inflamed that they bleed.
This is not usually serious in a UTI and responds quickly to antibiotic treatment but sometimes blood in the urine may indicate other problems. These include a kidney stone where pain in the loin or between the loin and groin is the predominant symptom. Blood in the urine without any pain needs exclusion of the possibility of a tumour in the bladder or kidney. Any person reporting painless haematuria should be advised to see their GP urgently.
Cloudy urine: Urine that is cloudy to the naked eye is an important diagnostic feature that may indicate antibiotic treatment. It is mainly caused by an excess of white blood cells in reaction to infection. Women may report that their urine appears cloudy. They may notice a change in appearance or odour on using the toilet.
Ideally, all patients should be asked to provide a sample of urine, if practicable, so that it can be assessed for cloudiness. The Pharmacy First clinical pathway calls for a “visual inspection by the pharmacist if practicable”.
Vaginal discharge: Absence of vaginal discharge is a key feature of acute uncomplicated cystitis: 80 per cent of women with vaginal discharge and symptoms of cystitis do not in fact have a UTI.
The presence of vaginal discharge may indicate a local fungal infection (usually candida or referred to as thrush), trichomoniasis or bacterial infection that would require referral. Vaginal pruritus or discharge may suggest vaginitis.
The sexually transmitted infection chlamydia is most commonly seen in women aged 16-24 years. About one in 10 women under the age of 25 years may have it. Unfortunately, about 80 per cent of women who have this infection are asymptomatic.
Those who do display signs can have symptoms of cystitis, an alteration in vaginal discharge or lower abdominal pain. Chlamydia can cause pelvic inflammatory disease (PID) and infertility, so it is important that the infection is detected and treated. Screening programmes for chlamydia are now widespread.
Other symptoms: Cystitis may be accompanied by suprapubic (lower abdominal) pain and tenderness.
Previous episodes: Women with recurrent UTIs (more than two episodes in the last six months or more than three in the last year) should be referred to their GP.
Diabetes: Recurrent UTIs can sometimes occur in diabetes – so anyone describing a history of increasing thirst, weight loss and a higher frequency of passing urine than normal should be referred. In patients with known diabetes and recent onset of urinary symptoms, it is best that they are assessed at the GP surgery as UTIs can be more troublesome and sometimes difficult to treat.
Post-sex cystitis: Sexual intercourse may precipitate an attack of cystitis due to minor trauma or resulting infection when bacteria are pushed along the urethra. The occurrence of urinary symptoms after starting a new sexual relationship is still sometimes referred to as ‘honeymoon cystitis’.
Postmenopausal women: Oestrogen deficiency in postmenopausal women leads to thinning of the lining of the vagina. Lack of lubrication can mean the vagina and urethra are vulnerable to trauma and irritation, and attacks of cystitis can occur. There may be other symptoms, such as hot flushes and night sweats.
Medication: Cystitis can be caused by cytotoxic drugs, such as cyclophosphamide. Other drugs, such as opioids and nifedipine, can also cause urinary tract symptoms.
Irritants: Other precipitating factors may include the irritant effects of toiletries (e.g. bubble baths and vaginal deodorants) and other chemicals (e.g. spermicides and disinfectants). Use of a diaphragm for contraception can also cause cystitis symptoms. However, lack of personal hygiene is not thought to be responsible for this problem, except in extreme cases.
Urine testing: Dipstick testing or sending a urine sample for culture are used only in specific circumstances and in the Pharmacy First clinical pathway in England would only apply to women referred to general practice (see TARGET flowchart for women under 65 years with suspected UTI).
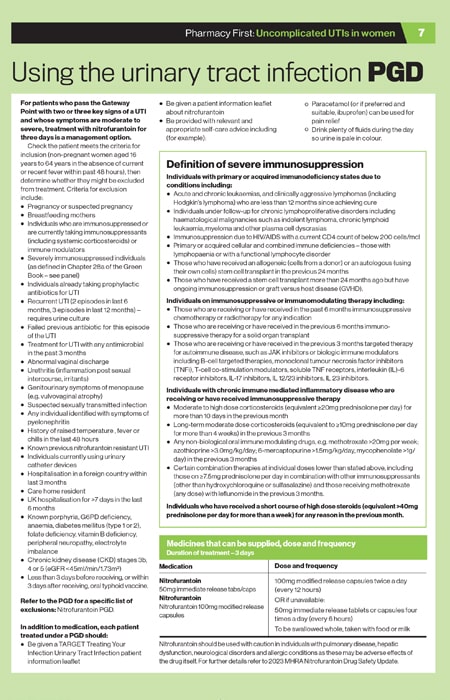
The patient group direction for the Pharmacy First service gives specific inclusion and exclusion criteria. The following is intended to give some practical guidance on how these might be followed – it is not intended to be definitive.
Most of the people who attend a pharmacy with cystitis will have pain but are not severely ill.
A few patients may attend who have symptoms suggesting more severe illness or who are at risk of severe illness. The most important requirement is to recognise severely ill patients and ensure they get urgent care. This might be facilitated by discussing with local GP practices in advance about how best Pharmacy First patients can access urgent assessment, if required.
Some patients may seek assessment but do not meet the inclusion criteria for the PGD under which the pharmacist is operating. These patients will need referral to their GP practice (or for urgent care, if required). The main complication of lower UTIs is ascending infection, which can lead to pyelonephritis and renal damage.
Same day
Less urgent referral (if obviously unwell/distressed may need same day)
Reflection exercise: Make contact with your local GP practice/s and share the list for urgent/ same day referral and less urgent referrals with them. Discuss how you will jointly manage this to ensure timely medical assessment.
Having established that a UTI is likely, the next decision is whether to suggest use of an antibiotic.
If symptoms are mild, then it is reasonable to discuss pain relief and give self-care advice to the patient. Offer paracetamol (or ibuprofen if preferred and suitable) for up to two days.
NICE advice is to encourage intake of enough fluids to avoid dehydration, but not to recommend cranberry products (although they may have a role in prevention) or urine alkalinising agents for symptom relief.
In cases of uncomplicated UTIs in women who have all three key features – dysuria, new nocturia and cloudy urine – it is no longer routine to send urine for culture and antibiotics are used empirically.
The PGD for the Pharmacy First service is to use nitrofurantoin. There may be a local policy in line with regional sensitivity data, which in some areas may recommend trimethoprim, so this should be consulted.
Acute, uncomplicated UTI usually resolves within a few days with or without antibiotic treatment. The duration of a UTI treated with an antibiotic to which the pathogen is sensitive is around 1.5 days shorter than when not treated with an antibiotic (3.3 vs 4.9 days).
If symptoms have not subsided within two days of beginning treatment, or have got worse, the patient should attend their general practice.
In addition to antibiotic treatment, it is important to offer advice about fluid intake. For women in whom cystitis is a recurrent problem, self-help measures can sometimes prevent recurrence. Signposting to relevant lifestyle information is useful.
Potassium and sodium citrate
Potassium and sodium citrate work by making the urine alkaline and have traditionally been used for cystitis. The acidic urine produced as a result of bacterial infection is thought to be responsible for the dysuria: alkalinisation of the urine may help to relieve discomfort, although there is no strong evidence of its benefit.
In the absence of evidence of effectiveness, NICE Clinical Knowledge Summaries (CKS) advises against recommending urine-alkalinising agents.
Patients may have used these before and may wish to purchase them. Anyone taking potassium-sparing diuretics, aldosterone antagonists or angiotensin- converting enzyme inhibitors should not use potassium citrate because it may cause hyperkalaemia. Sodium citrate should not be recommended for hypertensive patients, anyone with heart disease or pregnant women.
Self-care advice advice for a UTI is also relevant for preventing future episodes. Around 25-35 per cent of women with a UTI have a recurrent infection with three to six months and over 40 per cent within 12 months.
• Drink enough fuids: During a UTI patients may avoid drinking fluids because passing urine is painful. NHS advice is to “rest and drink enough fluids so you pass pale urine regularly during the day”. Current advice is to remain well hydrated (but not to deliberately increase consumption). This is important, especially during warmer weather.
• Empty the bladder completely when passing urine: Wait for 20 seconds after passing urine and then strain to empty the final drops. Leaning backwards is said to help to achieve a more complete emptying of the bladder compared with the usual sitting posture.
• Wipe front to back after a bowel motion: This may help to minimise transfer of bacteria from the bowel into the vagina and urethra. However, NICE advises that evidence is lacking.
• Go to pass urine after having sex: Urination immediately after sexual intercourse will theoretically flush out most bacteria from the urethra, but there is no evidence to support this.
• Wash the external vaginal area before and after having sex: This will wash away any bacteria that might be near the urethral opening.
• If post-menopausal: Where vulvovaginal atrophy is an issue, vaginal oestrogen pessaries may help.
• Complementary therapies: There is limited evidence that cranberry products and D-mannose can help to prevent UTIs (but no evidence that they can manage symptoms).
• Reduce intake of coffee and alcohol: This may help because they seem to act as bladder irritants in some people.

Case Study
Bina, aged 27 years, has asked for your advice at the pharmacy. She thinks she has a urinary tract infection as it is painful when she urinates.
1. What other signs and symptoms mean that a UTI is likely?
a) Cloudy urine
b) Blood in the urine
c) Vaginal discharge
d) Frequency
Bina tells you that she has also been going to the loo more frequently and often at night.
2. What are the options at this stage?
a) Refer Bina to GP practice
b) Refer Bina to a sexual health clinic
c) Advise her that she needs an antibiotic
d) Take a shared decision-making approach to decide on the course of action
Because of the severity of Bina's symptoms, you agreed to provide a course of antibiotics.
3. What is the most appropriate option?
a) Trimethoprim 200mg twice daily for 5 days
b) Trimethoprim 200mg twice daily for 3 days
c) Nitrofurantoin 100mg twice daily for 3 days
d) Nitrofurantoin 100mg twice daily for 5 days
MCQs
4. How should you manage women with 2 or 3 of the key symptoms?
a) Refer them to GP practice
b) Offer nitrofurantoin treatment if symptoms are moderate to severe
c) Provide self-care advice if symptoms are mild
d) Use a shared decision-making approach
5. In which of the following circumstances would it be appropriate to offer a course of nitrofurantoin?
a) If vaginal discharge is present
b) The woman has none of the key diagnostic criteria
c) The woman has more than 1 of the key diagnostic criteria
d) There is frequency, urgency and visible haematuria
6. Which signs and symptoms are associated with uncomplicated UTI?
a) Fever
b) Dysuria
c) Loin pain
d) Nocturia
7. What are the 3 key diagnostic criteria for UTI?
a) Haematuria, flank pain, frequency
b) Suprapubic tenderness, urgency, vaginal bleeding
c) Dysuria, new nocturia, cloudy urine
d) Vaginal dryness, vaginal irritation, itching
8. Which of the following are inclusion criteria for the UTI patient group direction (PGD)?
a) Non-pregnant females aged 16-64 years
b) Informed consent
c) Men aged 16 to 64 years
d) Non-pregnant females aged 18-54 years
Case study and questions provided by Agilio, author of NICE Clinical Knowledge Summaries (CKS), which has developed free Pharmacy First e-learning courses. Register at https://learn.clarity.co.uk/Courses/pharmacy-first
Useful resources
NHS Pharmacy First service specification, clinical pathways and PGDs
Community Pharmacy England
NHS Health A-Z UTIs
RCGP TARGET antibiotics toolkit hub
NICE CKS: Urinary tract infection (lower) – women
Note: For a comprehensive compendium of useful service and clinical resources, see online version of this Pharmacy First toolkit at Pharmacy Magazine
Back to top
![]()
Key information from patient history
Emergency or GP referral (direct referral to A&E if severely ill)



{kind=link}
{kind=link}
{kind=link}
{kind=link}