Pharmacy First Toolkit: Acute otitis media
Sonya Reuther,
04 Feb 2025![]() 20 Min
20 Min
This site is intended for Healthcare Professionals only
Sonya Reuther,
04 Feb 2025![]() 20 Min
20 Min
Sonya Reuther,
04 Feb 2025![]() 20 Min
20 Min
The Pharmacy First service in England allows community pharmacy teams to complete episodes of care for seven common conditions.
This Toolkit is designed to support pharmacists and their teams deliver Pharmacy First services in the UK for acute otitis media (AOM). It covers:
Dowload the toolkit pdf here.
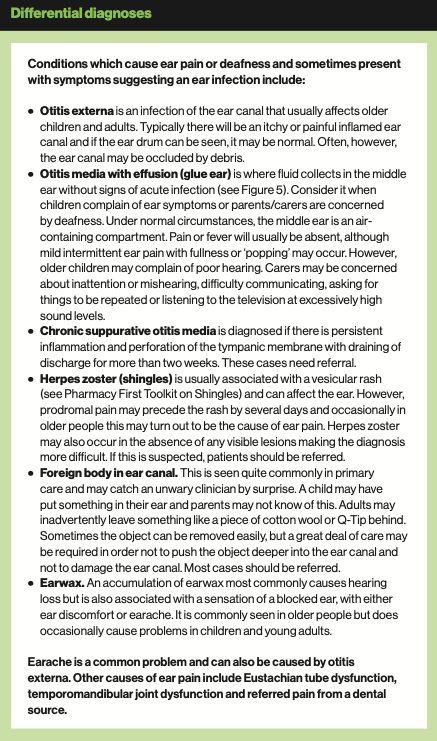
Earache is a frequent accompaniment to colds, especially in young children. When inflammation, nasal mucus and congestion are present in the upper respiratory tract, the ear can feel blocked and may feel uncomfortable or painful. This is due to inflammation of the throat and nasal passages and associated blockage of the Eustachian tube, which connects the middle ear to the back of the nasal cavity.
If the Eustachian tube is blocked, the ear can no longer be cleared or air pressure equalised through swallowing, which may make the patient feel uncomfortable and deaf. Sometimes, the middle ear fills up with fluid and is under pressure. It can become acutely painful (otalgia) but normally resolves spontaneously. It is common in young children and usually the best treatment is pain relief medication.
A secondary infection with inflammation may follow – this is acute otitis media – and the evidence shows that, for many young people, antibiotics only make a small difference in resolving symptoms, which usually settle within a week. Resolution occurs naturally when the blocked Eustachian tube reopens and the middle ear drains.
Antibiotics provide most benefit in children under two years of age who have pain in both ears, or in those with a painful ear with discharge (i.e. otorrhoea following ear drum perforation). Despite this, around 60 per cent of children with symptoms of AOM receive antibiotics in the UK. The condition has become less common in recent years; this may be due to the use of pneumococcal vaccine in children.
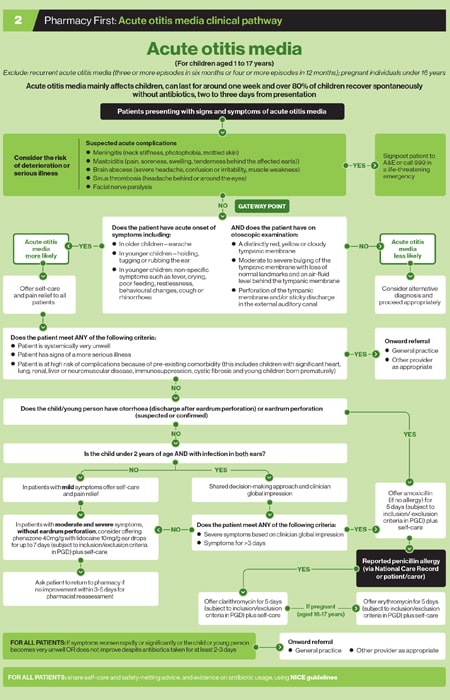
Use the clinical pathway for AOM to help guide your decision-making. The Pharmacy First service in England is intended for children aged from one to 17 years, but those with recurrent AOM (three or more episodes in six months or four or more episodes in 12 months), and pregnant individuals under 16 years of age, are excluded.
Download a PDF of the Accute Otis Media clinical pathway here or see below:
Age
For Pharmacy First in England, individuals under one year of age or over 17 years with suspected AOM and significant pain should be referred to their GP. This also applies to females who are pregnant (or with suspected pregnancy) under 16 years of age.
Association with viral respiratory infection
Acute onset of symptoms
A child who is screaming and distressed may settle quickly when the ear starts to discharge pus.
Recurrent AOM
Before any examination of the patient, consent should be sought. Hand washing is also required. It is good practice to check for a raised temperature using a thermometer.
Younger children may not have a clear cause for being miserable and unwell other than symptoms and signs of a respiratory infection, so it may be necessary to do an overall assessment and examine the throat at the same time.
Learning to examine the ear using an otoscope ideally requires supervised training. The more this is practised, the more competent a clinician will be. A normal ear drum (Figure 2) is translucent and greyish in colour.
Practise on staff or family (with their consent) to become familiar with using an otoscope and understanding what a normal ear drum looks like. There are some useful training resources available; for example, videos on the BMJ Learning website.
Examining children can be difficult particularly if they are fractious or unwell, and they may not co-operate. There are various techniques for reassuring the child and helping them feel more secure and at ease. If the carer or parent is confident in your approach, the child will usually be reassured that examination is a normal and necessary activity, as they will have learned to trust their carer/parent’s judgement.
The child may have play-acted such activities using a toy doctor’s kit. One tip is to introduce the suggestion that the examination is fun, like play-acting, especially in children over three years of age. Another is to ask if there is light coming out of the other ear. These small things can make a big difference.
The child should sit on an adult’s lap, held sideways for examining the ears. Both the child’s hands should be secured by the adult with one hand, the head held firmly against the chest with the other. The otoscope should be held lightly, like a pencil between thumb, index and middle fingers, left hand for left ear and right hand for right ear.
The little finger can be rested on the forehead or cheek, acting as a pivot, providing support and allowing movement of the head without knocking the ear canal, which is sensitive. Repeat with the head held the other way for the other ear.
Increasingly, fibre optic digital otoscopes are being used rather than the traditional optic lens devices. These connect to smart phones or tablet devices via Bluetooth or wi-fi, or are attached directly to the phone, so the ear drum can be visualised on screen. They have a wide angle of view at the tip and are generally easier to use and less invasive.
The main impediments to seeing the ear drum clearly are debris or inflammation of the ear canal (usually due to otitis externa), or wax. Wax appears as a yellowy, orange or brown deposit. If the ear drum has perforated due to infection, there may be pus in the ear canal – usually yellow or green (see Figure 6). Acute otitis media is confirmed, and the Gateway Point reached, if an otoscopic examination reveals:


Don’t be surprised if you encounter a foreign body in the ear canal in younger children or even in adults.

Taken from CPPE’s assessment record on Clinical Examination and Procedural Skills, February 2023
Most people who attend a pharmacy with ear pain or AOM will be unwell and have pain but are not severely ill. A few patients may attend who have symptoms suggesting more severe illness or who are at risk of severe illness.
Before carrying out an otoscopic examination, consider the risk of the patient’s condition deteriorating or indeed whether a more serious illness might be present. The most important requirement is to recognise when patients are severely ill and make sure they get urgent care.
Severe complications of AOM are rare. However, the following should be referred urgently – call 999 or go straight to A&E. Individuals with:
The PGD's also list the following, where the urgency of patient referral will be determined by their clinical condition. Pharmacists will need to use their professional judgement and be aware that these lists are not inclusive:
Pain relief with paracetamol or ibuprofen
This is advised for all patients with ear pain, whether an antibiotic is supplied or not. Patients should be offered regular doses of paracetamol or ibuprofen. It is important to use the right dose for the age or weight of child, and to use the maximum doses for severe pain.
Use of the TARGET leaflet: Respiratory Tract Infections is advised to support patients, particularly if antibiotics are not used (See Royal College of General Practitioners website).
When NICE reviewed the evidence for pain relief in AOM, they found that paracetamol and ibuprofen were both more effective than placebo in reducing pain at 48 hours in children with the condition, with a number needed to treat [NNT] of 6 to 7 for no pain at 48 hours.
Paracetamol and ibuprofen appeared to be equally effective, both for relieving pain and reducing fever. There is only limited evidence that combining paracetamol and ibuprofen is more effective than using paracetamol alone.
Phenazone and lidocaine ear drops (Otigo)
Another option in the NICE AOM guideline is to offer the combination of phenazone with lidocaine ear drops (Otigo) for pain. Phenazone is a form of non-steroidal anti-inflammatory drug. This change in guidance in 2022 was based on the new product becoming available. It may be considered as an alternative to antibiotics and may help reduce antimicrobial resistance.
The clinical pathway advises that phenazone with lidocaine should be considered in patients with AOM on otoscopic examination and with moderate or severe symptoms without eardrum perforation. It can be used for up to seven days.
Advice should be given to return to the pharmacy if there is no improvement in three to five days for reassessment. If the person becomes systemically very unwell, they should seek medical advice.

There is some debate about whether the evidence on efficacy and safety is adequate to support the change in guidance, which was based on one Cochrane systematic review (2011) and one subsequent clinical trial (2019).
The Cochrane review included five trials, involving 391 children and a variety of different ear preparations, and concluded that further high-quality, randomised, placebo-controlled trials were needed to establish more clearly the safety and efficacy of analgesic drops for AOM.
The more recent clinical trial involved 106 children. The authors concluded that the effects on pain were not clear and that the outcome of reduced antibiotic consumption required replication in a larger study.
Prescribing of Otigo in primary care has been low so far, with an estimated 30,000 prescription items written by GPs in England in 2023.
Decongestants and antihistamines
NICE does not advise decongestants and antihistamines since the evidence suggests they do not relieve symptoms.
Antibiotics
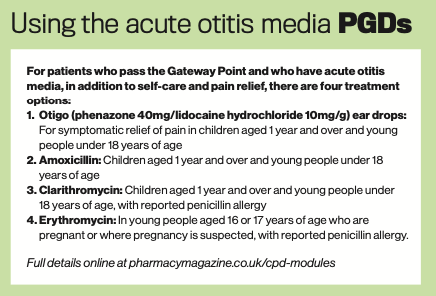
Under the clinical pathway there are two main groups eligible for antibiotic provision by a pharmacist.
1. People under the age of 18 who have otorrhoea (discharge after eardrum perforation) or eardrum perforation (suspected or confirmed).
2. Children under 2 years with infection in both ears diagnosed via otoscopy with severe symptoms and symptoms that last for three or more days.
In children under two years with bilateral AOM whose symptoms are not so severe, or do not appear particularly unwell, watchful waiting for between three to five days and possible use of phenazone with lidocaine is advised.
Amoxicillin is the recommended first-line antibiotic. Clarithromycin can be offered if there is a history of penicillin allergy stated by the patient/ carer or recorded on the NHS national care record. Erythromycin is an option in pregnancy or suspected pregnancy in the context of penicillin allergy.
Despite being used by GPs in up to 60 per cent of AOM cases, antibiotics have limited benefits. A Cochrane review showed that without antibiotic treatment, symptoms improved within 24 hours in 60 per cent of children and settled spontaneously within three days in 80 per cent.
Antibiotics also did not significantly reduce pain at 24 hours compared with placebo. Antibiotics did significantly reduce pain at two to three days, but the absolute difference was small: 88 per cent of children had no pain in the antibiotic group compared with 84 per cent in the placebo group.
Some children may benefit more than others and subgroup analyses showed that children under two years with bilateral acute otitis media had a NNT of 4 for earlier symptom resolution. Children with acute otitis media and otorrhoea had a NNT of 3 for earlier symptom resolution.
Common complications of acute otitis media are recurrence of infection, hearing loss (usually temporary) and perforated eardrum. Antibiotics were found to make little difference in preventing these.
Acute complications of AOM, such as mastoiditis, meningitis, intracranial abscess, sinus thrombosis and facial nerve paralysis, are very rare. There is limited evidence that these can be avoided by antibiotic use.
Any benefits of antibiotics must be weighed against the possible harms. The Cochrane review found that for every 14 children treated with antibiotics, one child experienced an adverse event (such as vomiting, diarrhoea or rash) that would not have occurred if antibiotics were not given.

Case study
Courtney is a 4-year-old girl brought to see you on a Monday morning by her grandmother. She has a raised temperature, loss of appetite and has been crying. On examination, her temperature is 37.6°C, pulse is 88 beats per minute. Her throat looks slightly red, as does her left tympanic membrane.
1. Which of the following are reasonable next steps in her management?
a) Offer a review within 72 hours if 3 she is not feeling any better and provide advice about regular analgesic use
b) Offer an antibiotic
c) Advise the grandmother to make an appointment for Courtney with the GP
d) Offer ear drops containing an anaesthetic and analgesic for pain
You agree that you will review Courtney in 72 hours and provide advice about pain relief in t he meantime. She re-attends with her father on Wednesday. He tells you that she is no better and that her temperature is high in the 4 evenings, she is still not eating and is crying persistently.
Courtney’s throat is still red and her left tympanic membrane is now perforated. Her temperature is 37.80C and pulse reads 82bpm.
2. Which of the following are now reasonable next steps in her management?
a) Advise further pain relief and review in 48 hours
b) Offer a course of amoxicillin
c) Advise the father that he should take Courtney to A&E
MCQs
3. What information and advice should you provide to Courtney’s father about acute otitis media?
a) The usual course of acute otitis media is about three days, but can be up to one week
b) Decongestants or antihistamines 6 can help manage symptoms
c) Symptoms should start to improve within three to five days of starting the antibiotic
d) They should seek medical help if symptoms worsen rapidly or significantly or do not improve after completion of treatment
4. Which of the following are inclusion criteria for the PGD?
a) People aged over 18 years
b) People aged under 18 years with otorrhoea
c) Children aged over 1 year but under 2 years with bilateral symptoms for more than 3 days
d) Children aged under 1 year
5. Acute otitis media is common:
a) In children
b) In people with immunodeficiency
c) In a household where people smoke
d) In all of the above
6. Those patients who most benefit from antibiotics for acute otitis media include:
a) A child with bilateral infection
b) A child under the age of 2 years of age
c) A child with otorrhoea
d) All of the above
7. Which of the following are exclusion criteria for the PGD?
a) People who are immunosuppressed
b) People who are severely immunosuppressed
c) Children with bilateral acute otitis media and severe symptoms
d) Failed previous antibiotic for this episode of acute otitis media
Answers: 1. a, d 2. b 3. a, c, d 4. b, c 5. d 6. d 7. a, b, d
Case study and questions provided by Agilio, author of NICE Clinical Knowledge Summaries (CKS), which has developed free Pharmacy First e-learning courses. Register at: https://learn.clarity.co.uk/Courses/pharmacy-first
Back to top
![]()



{kind=link}
{kind=link}
{kind=link}