Pharmacy First Toolkit: Impetigo
Sonya Reuther,
04 Feb 2025![]() 15 Min
15 Min
Sonya Reuther,
04 Feb 2025![]() 15 Min
15 Min
Sonya Reuther,
04 Feb 2025![]() 15 Min
15 Min
The Pharmacy First service in England allows community pharmacy teams to complete episodes of care for seven common conditions. This service toolkit provides an overview of the clinical pathway, protocol and PGDs used to deliver consultations on impetigo plus essential information to aid clinical decision making.
This toolkit is designed to support pharmacists and their teams to deliver the Pharmacy First and similar services in the UK for impetigo. It covers:
After reading the toolkit you will be able to assess the skin appearance and relevant history to decide whether impetigo is present; be able to decide whether antibiotic or symptomatic treatment is required; and know which conditions and red flags require referral.
Download the Toolkit PDF here.
Impetigo is a common skin infection, especially in young children. Parents may attend the pharmacy with their child, concerned that it is a serious or worrying condition such as scabies or cellulitis. They may also worry whether the child has an underlying skin condition such as eczema.
Most impetigo cases are uncomplicated but highly infectious. They can usually be managed with a short course of topical hydrogen peroxide or a topical antibiotic. Only more severe or complicated disease will require oral antibiotic treatment.
It is important to reassure parents once you are confident of a diagnosis, as it is usually a simple condition to treat (although, as ever, children with immunosuppression should be treated with caution).
Impetigo is caused when bacteria enter the skin through breaks caused by minor trauma such as insect bites or scratches, or underlying skin conditions such as eczema or scabies. The incubation period is 4-10 days.
There are two forms of impetigo – bullous and non-bullous. Non-bullous impetigo is caused by Staphylococcus aureus, Streptococcus pyogenes or a combination of both. Bullous impetigo is caused by Staphylococcus aureus. Impetigo caused by methicillin-resistant Staphylococcus aureus (MRSA) is becoming increasingly common.
Transmission occurs directly through close contact with an infected person or indirectly via contaminated objects such as toys, clothing or towels. Risk factors include skin trauma or pre-existing skin disease, hot/humid weather, poor hygiene and crowding.
Cases are most common in children aged between 0-14 years of age. Annual incidence is around 2.8 per cent in children up to 4 years of age and 1.6 per cent in children aged 5-15 years.
The most common form of the disease is non-bullous impetigo, which makes up approximately 70 per cent of cases and where large outbreaks can occur.
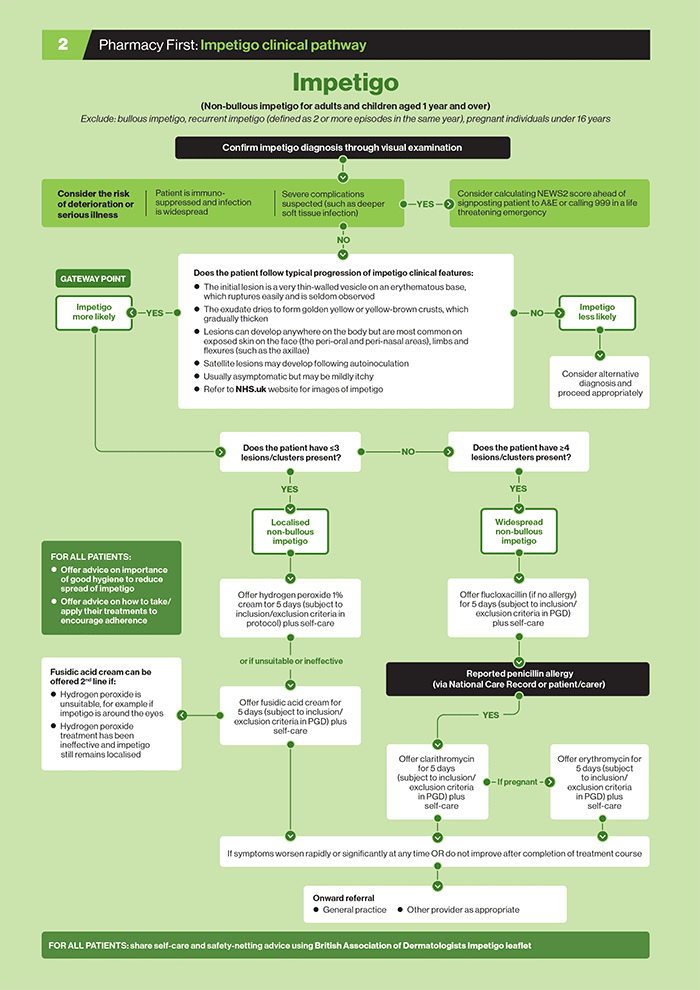
Download a PDF of the shingles clinical pathway here or see below:
Impetigo starts as small, thin-walled vesicles that burst quickly, leaving an exudate that dries to form a thick yellowish (honey-coloured) or brown crust. It is often described as looking like stuck-on cornflakes (see below).
Lesions typically appear on the face, around the mouth or nose, but can also occur elsewhere on the body (e.g. axillae or trunk). Lesions often occur in clusters and can coalesce. Satellite lesions can develop as a result of autoinoculation from scratching or touching the original lesions.
The crusts dry and heal without scarring over 2-3 weeks. There may be residual redness that fades over days or weeks. A diagnosis is usually based on the clinical appearance and history.
If there is damage to the skin – for example, due to eczema, scabies or insect bites (including head lice) – the impetigo may become more widespread as the damaged skin provides a portal for entry of bacteria.
Systemic symptoms are usually absent. Patients do not have sore throats but may have regional lymphadenopathy. There is usually little or no evidence of deep-seated infection (tissue inflammation, swelling or redness).
Bacterial culture is not routinely required unless there is recurrent or poorly responsive infection or methicillin-resistant Staphylococcus aureus (MRSA) is suspected.
The main risk factors for impetigo are young age (under 5 years), contact with other cases, and crowded living or work conditions.
When taking a patient history, ask about:
A visual examination should be sufficient to determine the nature and extent of the skin lesions. Look for the clinical features of impetigo and determine whether the lesions are those of localised or widespread, non-bullous impetigo:
Also check for features of systemic involvement such as fever, lethargy or feeling unwell.
Derived from training materials at www.rcgp.org.uk/targetantibiotics
The Pharmacy First (England) PGDs for impetigo list specific inclusion and exclusion criteria. Most patients with suspected impetigo will not be systemically unwell, but parents/guardians may be concerned about their child’s appearance.
A few patients may have symptoms suggesting more severe illness (e.g. painful, hot, swollen skin, and spreading redness) or be at risk of severe illness (e.g. immunosuppressed individuals). Some may not meet the Gateway Point under which the pharmacist is operating (such as those with recurrent or bullous impetigo). It is important to recognise severely ill patients and ensure they get urgent care.
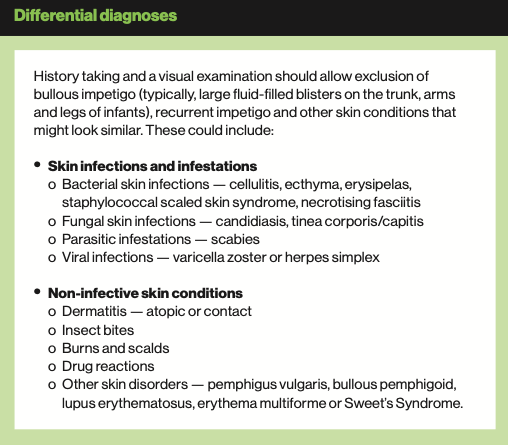
Complications with impetigo are uncommon. The Pharmacy First clinical pathway lists conditions for urgent referral: call 999 or send patients to A&E if sepsis or deeper soft tissue infection is suspected, or if the person is immunocompromised and infection is widespread.

Antibacterial treatment is recommended for impetigo to shorten the course of illness and reduce the chances of spreading it to other sites on the body or other people.
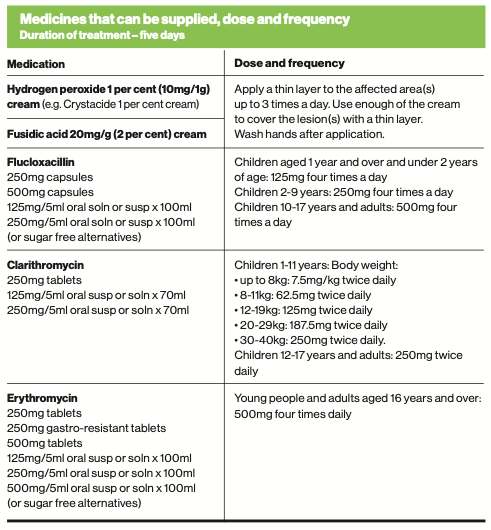
Topical treatment with a five-day course of hydrogen peroxide 1 per cent cream is first-line treatment for localised non-bullous impetigo. A five-day course of oral flucloxacillin is first-line treatment for widespread non-bullous impetigo.
If flucloxacillin is indicated, remember to check for penicillin allergy and supply an alternative (clarithromycin or erythromycin subject to inclusion/ exclusion criteria) if necessary.
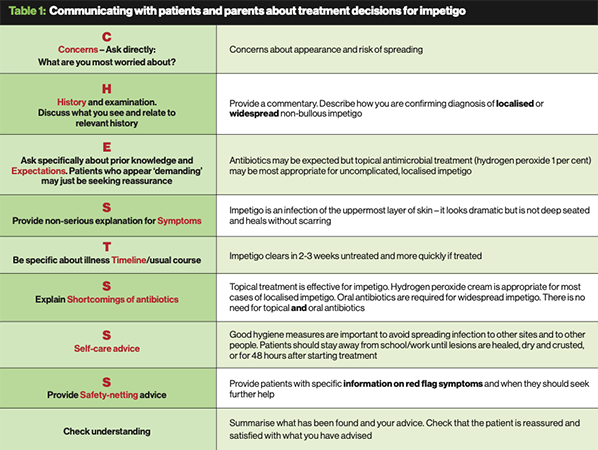
While antimicrobial treatment is appropriate for impetigo, patients/parents need to understand how to use the treatment correctly. The CHESTSSS consultation structure, developed by the Royal College of General Practioners, provides a useful framework.
A useful way to think about the consultation is to over the 3 E's – Empathise, Evaluate and Educate. Table 1 (above) shows how the CHESTSSS framework could be tailored to structure consultations about impetigo. This also provides an opportunity to educate patients about appropriate and effective use of antibiotics and to reinforce good antimicrobial stewardship.
Ensure that patients and parents/carers get the best out of treatment by providing self-car advice:
For patients in whom impetigo is likely and so pass the Gateway Point, there are two topical and three antibiotic treatment options:
• For localised non-bullous impetigo (three or fewer lesions/clusters present) in children over 1 year and adults who are systemically well and not at high risk of complications.
1. Hydrogen peroxide 1 per cent cream
2. Fusidic acid 20mg/g (2 per cent) cream – where hydrogen peroxide 1 per cent cream is unsuitable (e.g. impetigo around the eyes) or ineffective
• For widespread non-bullous impetigo (four or more lesions/clusters present) in children aged 1 year and over and adults who are systemically well and not at high risk of complications.
3. Flucloxacillin
4. Clarithromycin – where flucloxacillin is not appropriate due to hypersensitivity
5. Erythromycin – where pregnancy is suspected and where flucloxacillin is not appropriate due to hypersensitivity
Check the patient meets the criteria for inclusion, then determine whether they might be excluded from treatment. General criteria for exclusion include:
• Individuals under 1 year of age
• Pregnancy or suspected pregnancy in individuals under 16 years of age
• Currently breastfeeding with impetigo lesion(s) present on the breast
• Individuals who are immunosuppressed or are currently taking immunosuppressants (including systemic corticosteroids) or immune modulators
• Severely immunosuppressed individuals (as defined in Chapter 28a of the Green Book – see panel)
• Recurrent impetigo (two or more episodes in the same year)
• Failed previous topical or oral treatment (including antimicrobials) for the current episode of impetigo
• Currently active underlying skin condition (e.g. uncontrolled eczema or contact dermatitis, or current episode of scabies, chickenpox or eczema herpeticum)
• Any open wounds affecting the application area or the immediate vicinity
• Bullous impetigo (characterised by flaccid fluid-filled vesicles and blisters (often with a diameter of 1-2cm), which can persist for 2-3 days
• Systemically unwell
• Signs/symptoms of a more serious condition/illness (e.g. swelling, large blisters, pain, pus or spreading redness)
Additionally, for antibiotic PGDs:
• Hypersensitivity reactions (e.g. anaphylaxis) to beta-lactam or macrolide antibiotics
• Individuals following a ketogenic diet
• Previous or current known methicillin-resistant Staphylococcus aureus (MRSA) colonisation or infection
• Known or suspected liver disease
• Known chronic kidney disease (CKD) stages 4 or 5 (eGFR <30ml/min/1.73m2)
• Less than 3 days before receiving, or within 3 days after receiving, oral typhoid vaccine
Refer to the PGDs for a specific list of exclusions for:
In addition to medication, each patient treated under a PGD (or their parent/ carer) should be:
1. Given the appropriate medicine patient information leaflet
2. Provided with the British Association of Dermatologists Impetigo leaflet www.bad.org.uk/pils/impetigo
3. Signposted to NHS Health A-Z: Impetigo www.nhs.uk/conditions/impetigo
4. Offered self-care advice.
Impetigo stops being contagious:
a) 48 hours after starting to use hydrogen peroxide cream or antibiotics
b) When patches dry out and crust over.
To help stop impetigo spreading or getting worse while it is still contagious:
a) Stay away from school or work
b) Keep sores, blisters and crusty patches clean and dry
c) Cover them with loose clothing or gauze bandages
d) Wash hands frequently, especially after accidentally touching the area
e) Wash flannels, sheets and towels at a high temperature (at least 60 ̊C) with the addition of laundry bleach
f) Wash or wipe down toys with detergent and warm water if children have impetigo.
Do not touch or scratch sores, blisters or crusty patches
Do not have close contact with children or people with diabetes or a weakened immune system
Do not prepare food for other people (food handlers are required by law to inform employers immediately if they have impetigo)
Do not go to the gym or play contact sports such as rugby or football
Always use a clean cloth to dry the affected area if necessary
Individuals with primary or acquired immunodeficiency states due to conditions including:
Individuals on immunosuppressive or immunomodulating therapy including:
Individuals with chronic immune mediated inflammatory disease who are receiving or have received immunosuppressive therapy:
Individuals who have received a short course of high dose steroids (equivalent >40mg prednisolone per day for more than a week) for any reason in the previous month:
Case study
Gabriella, aged 8 years, has been brought in by her mum to see you, as she thinks her daughter has a skin infection on her arm.
1. On examination, you suspect she has impetigo. What features would mean that you need to refer Gabriella to hear GP practice?
a) If there are 4 or more lesions
b) If she is immunocompromised
c) If this is the first time she has had impetigo
d) If she has recurrent impetigo
2. Gabriella is not immunocompromised, this is the first time she has had impetigo and there are more than four lesions. What is the most appropriate management option?
a) Offer hydrogen peroxide 1 per cent cream
b) Offer a 5-day course of oral antibiotic
c) Provide information and advice
d) Other fusidic acid cream
3. Because Gabriela has widespread (4 or more lesions), you offer a course of oral flucioxacillin and provide appropriate information and advice. Which statements below are correct?
a) She should seek medical advice if symptoms worsen rapidly or significantly at any time or have not improved after the course has been completed
b) Impetigo is not contagious so there is no need to worry about it being transmitted to family members
c) Gabriella should stay off school until 48 hours after treatment has started
d) She should stop the course of antibiotics once symptoms improve
MCQs
4. What is the first-line treatment for localised impetigo?
a) Hydrogen peroxide 1% cream
b) Oral flucloxacillin for 5 days
c) Fusidic acid cream
d) Oral erythromycin
5. Which of the listed impetigo diagnoses and treatments are correctly matched?
a) Localised non-bullous impetigo – topical hydrogen peroxide 1% cream
b) Widespread non-bullous impetigo – topical fusidic acid cream
c) Widespread non-bullous impetigo – oral flucloxacillin
d) Mild localised non-bullous impetigo – fusidic acid cream
6. Which of the following correctly describes the clinical features associated with bullous and non-bullous impetigo?
a) In non-bullous impetigo lesions begin as thin-walled vesicles or pustules
b) In bullous impetigo lesions are restricted to the face
c) In non-bullous impetigo lesions are most common on the trunk
d) For both types of impetigo, healing usually occurs within 2-3 weeks without scarring
7. What length of course of antibiotics should be provided to treat impetigo?
a) 10 days
b) 7 days
c) 5 days
d) 3 days
8. Under what circumstances should patients be referred to their GP?
a) If they are aged under 10 years
b) If bullous impetigo is suspected
c) The person is immunosuppressed
d) The person is severely immunosuppressed
Case study and questions provided by Agilio, author of NICE Clinical Knowledge Summaries (CKS), which has developed free Pharmacy First e-learning courses. Register at https://learn.clarity.co.uk/Courses/pharmacy-first
Useful resources
NHS Pharmacy First service specification, clinical pathways and PGDs
Community Pharmacy England
NHS A-Z
Patient UK
British Association of Dermatologists
Clinical Knowledge Summaries, NICE, updated August 2023. Impetigo
Primary Care Dermatology Society – Impetigo
Note: For a comprehensive compendium of useful service and clinical resources, see online version of this Pharmacy First toolkit plus the CPD module at Pharmacy Magazine
Back to top
![]()





{kind=link}
{kind=link}
{kind=link}
{kind=link}